Do your duty, prepare for your departure.
Tl;dr: Our medical/care system is screwed, governments are all efficiency- and cost-obsessed. They’re fixated on ageing and on the explosion of the ‘economically inactive’ population. This system would like the idea of more people taking the voluntary way out.
Am I being neurotic? My concerns about the assisted suicide bill, currently in the UK Parliament, are not with the risk of coercion by family members or doctors or scumbags of one kind or another – although I’m quite sure this is a real risk.
I’m also not particularly worried about ‘the slippery slope’ or about the risk that old people might want to avoid becoming a ‘burden’ (isn’t that actually a perfectly legitimate reason to go?). My concern is much simpler. It’s about this system, a healthcare system that is less and less humane; more and more obsessed with measurement and control, with efficiency and throughput and the management of shrinking resources.
In this system – this diminished and dehumanised system – the pressure to move the sick and elderly, the incurable and the intractable (the awkward, the unemployable, the unproductive) along the expensive health and care timeline and onto the fast track, onto the slip-road out of here, is already enormous.
My grim suspicion is that there are managers and administrators and government ministers (not forgetting the management consultancies and insurers and private equity firms) who would quite like to speed things up a bit, to increase the system’s throughput, to just slightly improve the ratios.
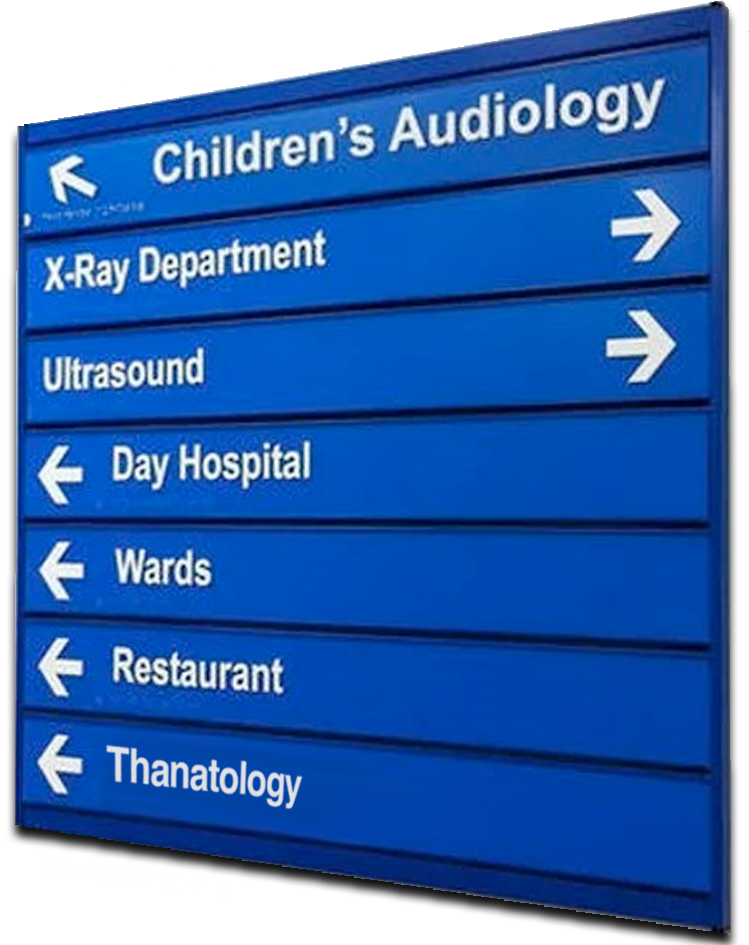
Thanatology? Just down the corridor
To deliver on this new policy, once it’s on the statute books, NHS managers will have to add death to the roster of treatments available and, presumably, add a Death Unit to every major hospital. They’ll mechanically formalise the process, setting targets and, quite plausibly, tweaking incentives to ‘nudge’ the sick and old onto the pathway. There can be no better way to address bed-blocking in our hospitals than by permanently removing the problem.
This system would like to reduce the pointless expenditure on keeping the sick and the inactive alive and to create in the citizenry – the customer-base, you and me – a new habit – the habit of volunteering to step off this mortal coil a bit early.
Not too early. Just a few months or a year. Barely noticeable, just a tiny statistical effect. But every little helps. Move along now. Off you go. Thank you for your contribution. It’s been lovely knowing you… See ya!
- I’m ready to make a small bet that within a few years we’ll see the first ‘Dignity Unit™’ or ‘Goodbye Suite™’ in the grounds of a hospital or a care home. It’ll be all pastel colours and there’ll be a wild-flower garden maintained by volunteers. A minor Royal will cut the ribbon…
- This, incidentally, explains why politicians are not freaking out about the fact that life expectancies are now falling in parts of the developed world – including Britain. That looks like a self-adjusting system to these people.